Why Am I Constipated?

Constipation is often defined medically as having fewer than three bowel movements per week, or experiencing symptoms such as hard stools, straining, or a sensation of incomplete evacuation.
These criteria are useful for identifying more severe constipation, but they do not always capture more subtle disruptions in digestive function.
In healthy digestive physiology, the coordinated movement of contents through the gastrointestinal tract typically leads to regular bowel movements. For many individuals, this occurs once per day, reflecting the normal daily cycle of digestion and intestinal propulsion.
Medical definitions of constipation usually focus on stool frequency and difficulty passing stool. While these criteria are useful, they do not fully explain why bowel movements become disrupted. From a physiological perspective, constipation can often be better understood as a breakdown in the coordinated propulsion of contents through the digestive tract.
Normal digestion depends on a sequence of carefully coordinated muscular contractions that move food and waste progressively from the stomach through the intestines and ultimately toward evacuation. When this coordinated propulsion becomes disrupted at any point along the digestive tract, bowel movements can become infrequent, difficult, or incomplete.
Constipation reflects a breakdown in the regulation and coordination of propulsion through the gastrointestinal tract.
Digestion normally depends on carefully regulated muscular contractions that move food and waste forward through the stomach, small intestine, and colon. These movements must occur in a coordinated sequence.
When this propulsion becomes disrupted — slowed, poorly coordinated, or obstructed — bowel movements can become infrequent, difficult, or incomplete.
Understanding where this breakdown occurs is often the key to understanding constipation.
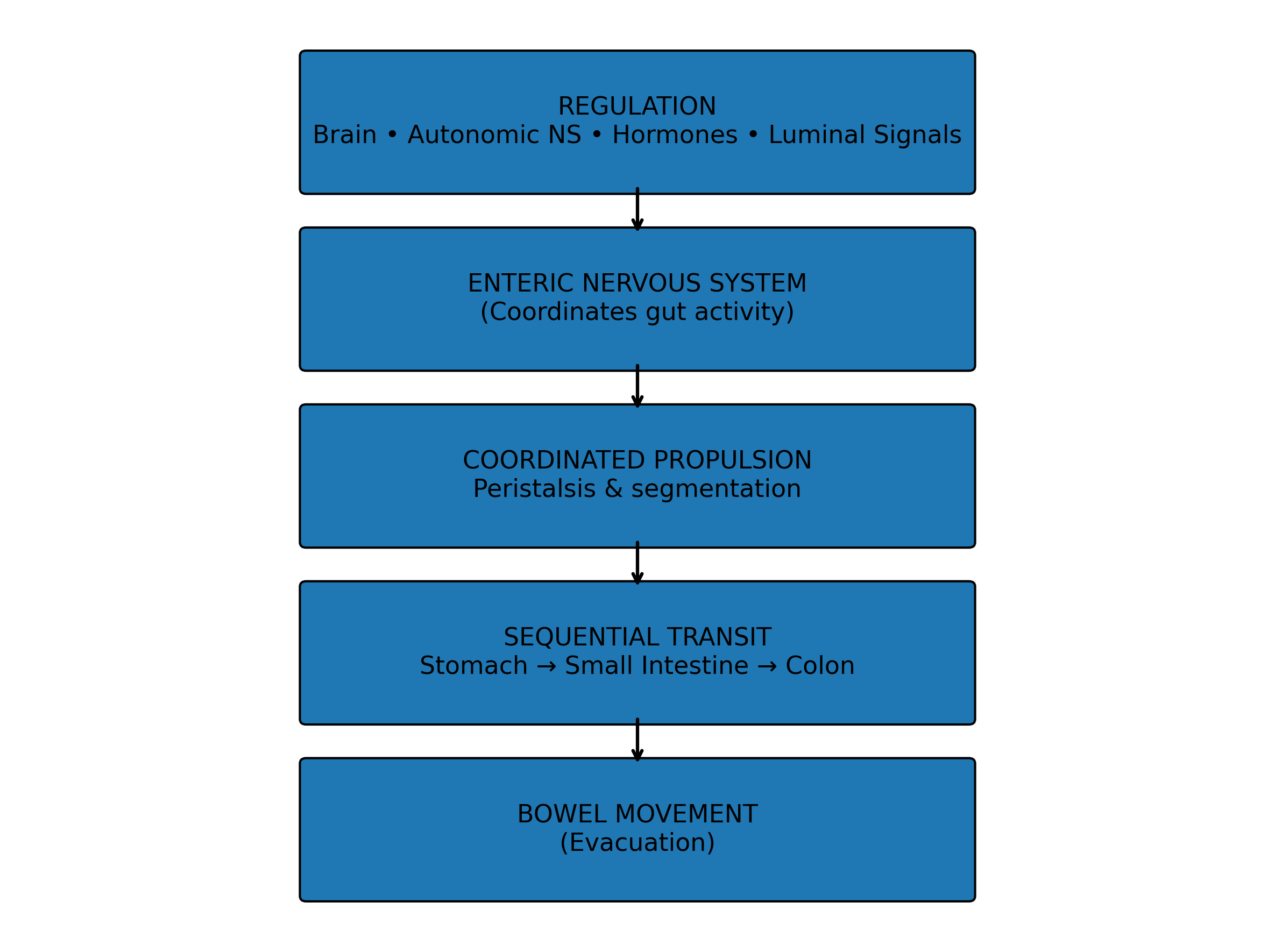
The diagram below illustrates the core process of digestive propulsion and how coordinated movement through the gastrointestinal tract ultimately leads to normal bowel function.
The diagram below illustrates how coordinated propulsion normally moves contents through the digestive tract.
Coordinated Propulsion in the Digestive Tract
Much of how I think about these patterns developed through hands-on clinical work with the structures of the digestive tract.
Over the past several years I’ve incorporated visceral manipulation and osteopathic-style manual assessment into my practice. Working directly with the tissues of the abdomen and pelvis has deepened my understanding of how the physical structures of the gut interact with nervous system signaling and luminal factors to influence movement through the digestive tract.
In practice, I’ve also found that hands-on work with the abdominal and pelvic structures is often one of the more reliable ways to help restore coordinated movement. It has also helped clarify the anatomical basis behind several of the acupuncture points traditionally used for digestive issues.
Common Reasons You May Be Constipated
Several systems must work together for normal bowel movements to occur. Constipation can develop when one or more parts of this digestive propulsion system becomes disrupted.
Slowed propulsion through the colon
Disruption of digestive motility, particularly in the stomach or small intestine
Changes in stool composition, including hydration, fiber, and microbial activity
Altered nervous system regulation, including stress or autonomic imbalance
Pelvic floor or outlet coordination problems, such as dyssynergic defecation
Because bowel function depends on the coordination of these systems, constipation often develops when one or more parts of this propulsion chain stop working effectively.
Where Propulsion Can Break Down
Constipation rarely results from a single cause. Instead, it often reflects disruption in one or more parts of the system that regulates digestive propulsion.
Digestive motility is influenced by a complex network of interacting factors, including nervous system regulation, hormones, luminal signals, and the intestinal microbiota. In this sense, bowel function reflects a complex and adaptive system.
At the same time, the physical movement of digestive contents follows a sequential path through the gastrointestinal tract. Food and waste move progressively from the stomach to the small intestine, through the colon, and ultimately toward evacuation.
Because of this directional flow, disturbances earlier in the digestive process can have downstream consequences. When digestion or propulsion is impaired upstream, the contents arriving later in the system may be poorly prepared for normal transit.
In other words, constipation can often be understood as a breakdown somewhere along the chain of coordinated propulsion.
For this reason, improving upstream digestive function can sometimes lead to improvements further along the digestive tract.
Below are some of the most common areas where coordinated propulsion through the gastrointestinal tract can become impaired.
Many different medical conditions, medications, and lifestyle factors can contribute to constipation. Although it is not possible to list every specific cause, most ultimately influence bowel function by affecting one or more of the propulsion mechanisms described below. In this way, constipation can often be understood as a disruption somewhere within the system that coordinates the movement of contents through the digestive tract.
The sections below follow the sequence of digestion, moving from upstream signals that initiate motility to the final coordination required for evacuation.
Initiation of Digestive Motility
The stomach also functions as an important regulatory gatekeeper for downstream digestive activity.
Stimulation of the stomach normally triggers reflexes that increase movement throughout the gastrointestinal tract. One example is the gastrocolic reflex, in which stomach activity stimulates contractions in the colon. Many people notice this effect after eating a meal, and substances such as coffee can provoke a particularly strong response in some individuals.
When the stomach becomes unusually sensitive or irritated, this reflex may become exaggerated, leading to urgency or rapid bowel movements.
The chemical environment of the stomach may also influence digestive signaling. Normal gastric acidity helps coordinate hormone release and downstream digestive activity. When stomach acidity is significantly reduced — for example through medications that suppress stomach acid or frequent use of antacids — digestive signaling may become weaker or less coordinated in some individuals.
Because the stomach sits at the beginning of the digestive process, disturbances in its signaling can sometimes influence bowel function further along the gastrointestinal tract.
Intestinal Propulsion
The small intestine and colon rely on coordinated muscular contractions to move contents forward through the digestive tract.
These movements are regulated by the enteric nervous system and by specialized pacemaker cells in the intestinal wall known as interstitial cells of Cajal, which help organize rhythmic patterns of contraction.
Although the small intestine and colon use somewhat different motor patterns, both depend on properly coordinated propulsion to move contents progressively through the gastrointestinal tract.
In the small intestine, motility primarily mixes and gradually advances digestive contents. When propulsion here becomes sluggish or poorly coordinated, food and digestive byproducts may remain in the small intestine longer than normal. This can lead to symptoms such as bloating soon after eating, abdominal distention, gas, or a sensation that food is “sitting” in the abdomen.
In contrast, when propulsion slows in the colon itself, stool may remain in the large intestine longer than normal. As water continues to be absorbed, stool becomes harder, drier, and more difficult to pass, producing the more familiar pattern of infrequent bowel movements and straining.
During fasting, digestive propulsion is also influenced by the migrating motor complex, a cyclic pattern of activity partly regulated by hormones such as motilin that helps move residual contents through the stomach and small intestine.
Disruption of these coordinated propulsion patterns can contribute to slower intestinal transit and the development of constipation.
Luminal Factors
The physical and chemical properties of intestinal contents play an important role in regulating digestive propulsion.
Normal intestinal movement is partly stimulated by luminal distention — the stretching of the intestinal wall as food, fluid, and stool move through the digestive tract. This distention helps activate the peristaltic reflex, allowing coordinated contractions to push contents forward.
When stool volume is too small, too dry, or poorly formed, this mechanical stimulus may be reduced. As a result, the signals that normally trigger intestinal propulsion can become weaker.
Hydration and dietary fiber both influence these physical properties. Fiber can help increase stool bulk and water retention, which may improve the mechanical signals that stimulate intestinal movement. However, the effects of fiber can vary depending on the type of fiber and the overall environment within the intestine.
Hydration and fiber also influence propulsion indirectly through their effects on the intestinal microbiota. These factors shape the composition and activity of gut bacteria, which in turn produce metabolic byproducts such as short-chain fatty acids and other signaling molecules that can affect intestinal motility.
In this way, both the physical characteristics of intestinal contents and the metabolic activity occurring within them can influence how strongly the digestive tract responds.
Some microbial products may stimulate intestinal propulsion and secretion, while others may slow movement through the gut. Because propulsion depends partly on the properties of the intestinal contents themselves, changes in diet, hydration, microbial activity, or stool composition can significantly influence bowel function.
Bile also contributes to the chemical environment of the intestinal lumen. Produced by the liver and released into the small intestine, bile acids help digest dietary fats and can influence intestinal motility and secretion. Changes in bile production, bile flow, or bile acid metabolism may alter the composition of intestinal contents and the signals that regulate propulsion. Bile acids also shape the intestinal microbiota by influencing which microbial species are able to thrive in the gut, while gut bacteria in turn modify bile acids through their own metabolic activity. In this way, hepatobiliary function can influence bowel habits both directly and indirectly through its effects on the luminal environment and the intestinal microbiota.
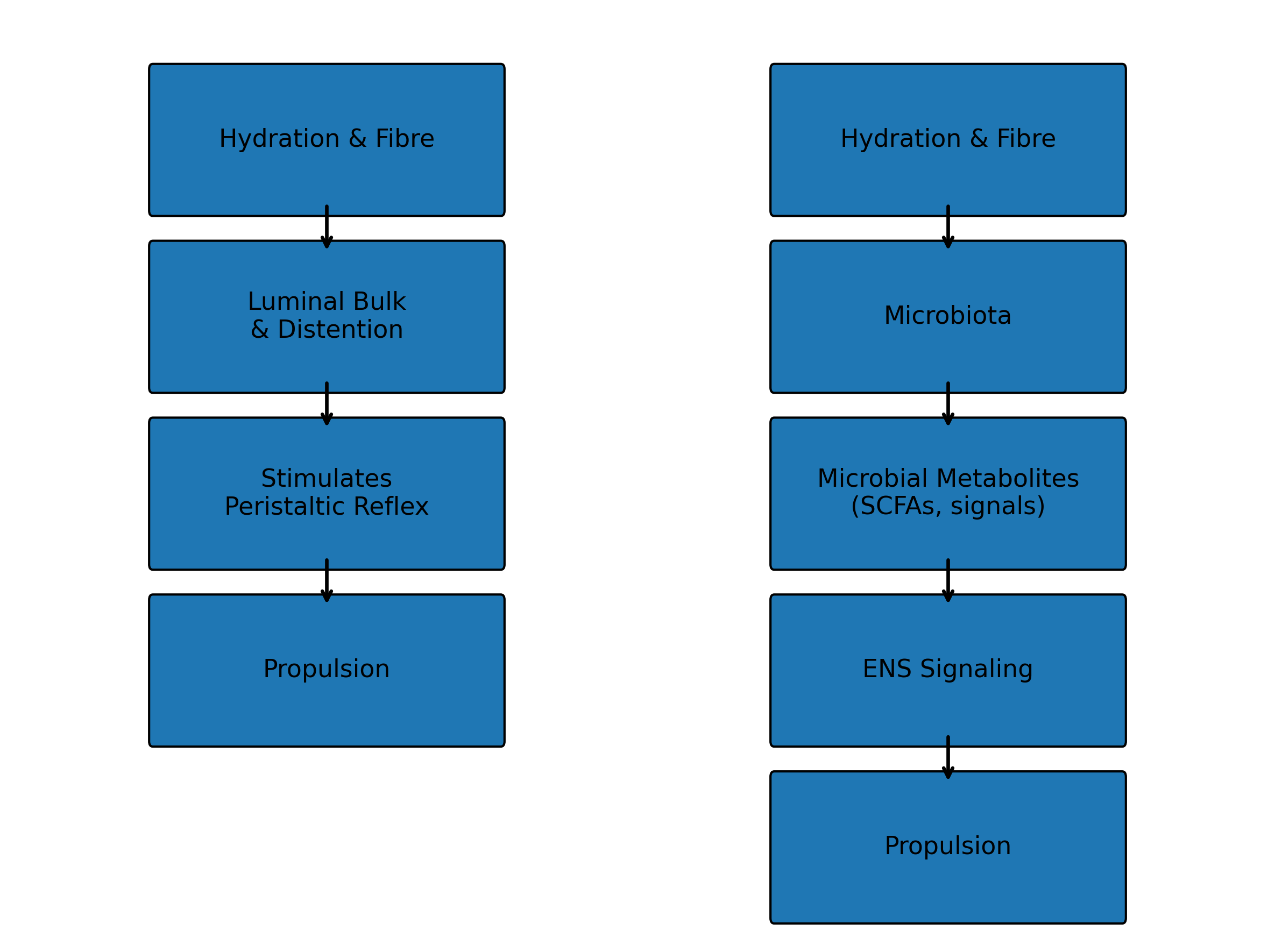
The diagram below illustrates how luminal factors such as hydration, fibre, and the intestinal microbiota influence intestinal motility and digestive propulsion.
Luminal Factors That Influence Intestinal Propulsion
Nervous System Regulation
Digestive propulsion is closely regulated by the nervous system.
The gastrointestinal tract contains its own network of nerves known as the enteric nervous system (ENS). This system coordinates many of the contractions that move food and waste through the digestive tract. A major component of this network is the myenteric (Auerbach’s) plexus, a layer of neurons located between the intestinal muscle layers that plays a central role in organizing the rhythmic contractions responsible for propulsion.
Although the ENS can function independently, it is also influenced by signals from the broader nervous system through the autonomic nervous system. Parasympathetic signals generally support digestive activity, while sympathetic signals associated with stress or threat can suppress digestive movement.
These signals help the body adjust digestive activity depending on circumstances. During periods of acute stress or heightened sympathetic nervous system activity, digestive propulsion may slow. In more relaxed physiologic states, digestive coordination is typically more active.
The close relationship between nervous system activity and digestive function is illustrated by therapies such as biofeedback, which can improve certain gastrointestinal conditions by helping individuals learn to regulate pelvic floor coordination and other physiologic responses involved in bowel function. Biofeedback is commonly used for disorders of defecation such as pelvic floor dyssynergia, and related behavioral approaches are also used in conditions such as irritable bowel syndrome (IBS) to help regulate communication along the gut–brain axis.
Communication between the digestive tract and the nervous system is also bidirectional. The intestinal microbiota produce signaling molecules that can influence nervous system activity and behavior, forming part of what is often referred to as the gut–brain axis.
In certain medical conditions, the enteric nervous system itself can be directly affected. Disorders such as Hirschsprung disease, diabetic neuropathy, and some forms of intestinal pseudo-obstruction illustrate how disruption of the neuromuscular signaling that coordinates intestinal contractions can impair digestive propulsion.
Certain medical conditions and medications can also influence digestive motility by affecting nervous system signaling or smooth muscle function within the digestive tract. For example, conditions such as hypothyroidism can slow metabolic activity and reduce intestinal propulsion. A number of medications — including opioid pain medications, some antidepressants, anticholinergic drugs, and certain blood pressure medications — may also contribute to constipation by altering normal motility patterns or intestinal secretions.
Because the nervous system plays a central role in regulating digestive propulsion, disturbances in autonomic balance, enteric signaling, or communication between these systems can disrupt the coordinated movement of contents through the gastrointestinal tract.
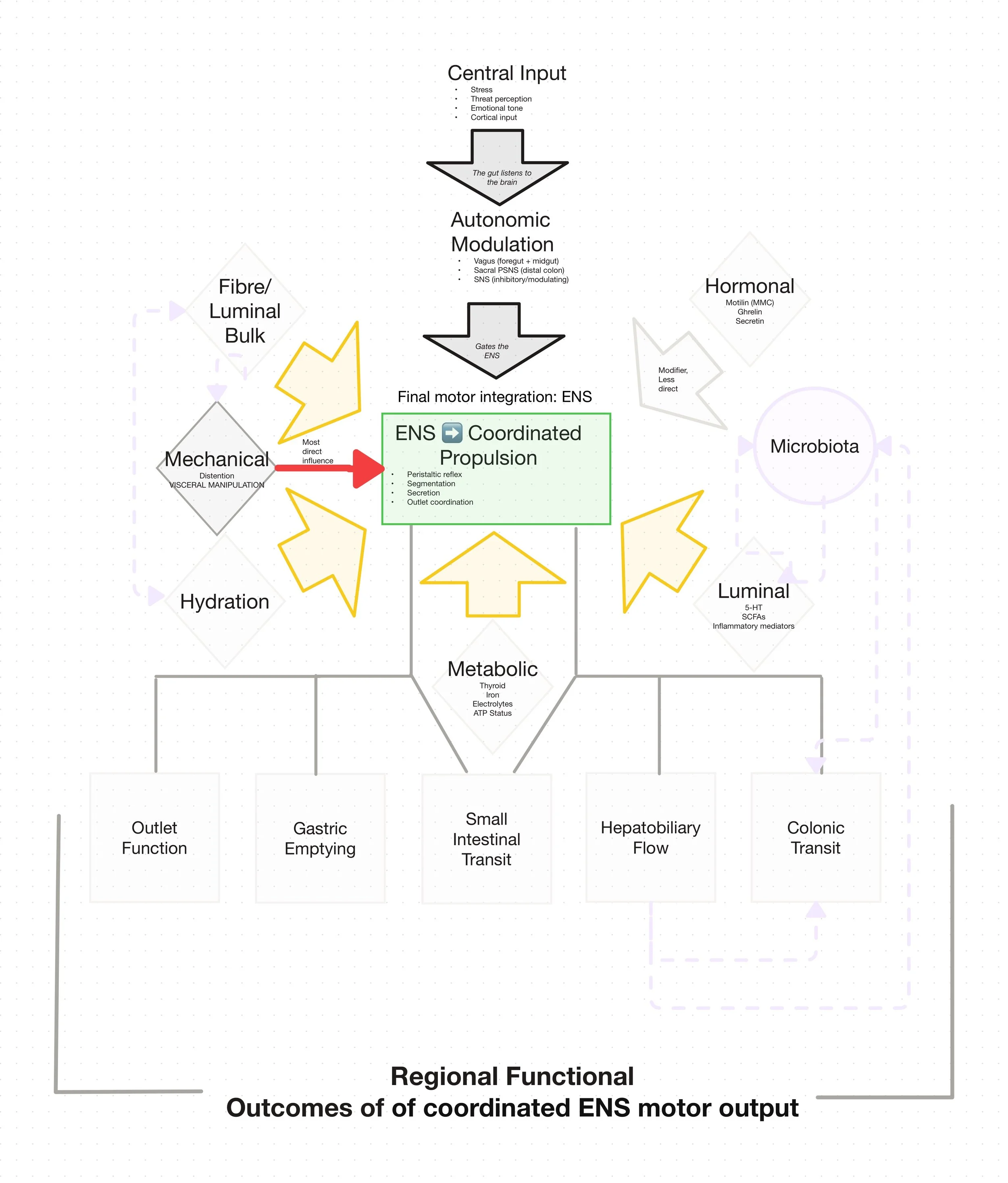
Many different systems influence how the gut moves. The diagram below shows how these inputs ultimately converge on coordinated propulsion within the gut.
How the Gut Coordinates Movement
Outlet Coordination
The final step in bowel function involves the coordinated relaxation and contraction of muscles in the rectum and pelvic floor.
As stool enters the rectum, stretch receptors signal that a bowel movement may be needed. In response, the rectum begins to contract while the muscles of the pelvic floor and anal sphincter relax, allowing stool to pass.
For a normal bowel movement to occur, these actions must happen in a coordinated sequence. When the rectum contracts and the pelvic floor muscles relax appropriately, stool can move downward and evacuation can occur.
If the urge to have a bowel movement is repeatedly ignored, the rectum can gradually adapt to the increased volume of stool. Over time the sensation of urgency may become weaker, and stool may remain in the rectum longer, allowing additional water to be absorbed and making evacuation more difficult. For this reason, consistently responding to the body’s natural urge to have a bowel movement can be an important part of maintaining normal bowel function.
In some individuals, however, the coordination between the rectum and pelvic floor becomes disrupted. The pelvic floor muscles may tighten instead of relaxing, or the timing of rectal contraction and sphincter relaxation may become poorly synchronized. When this occurs, stool may be difficult to pass even if it has moved normally through the rest of the digestive tract.
This pattern is often referred to as dyssynergic defecation or pelvic floor dysfunction.
People experiencing this type of constipation may describe symptoms such as:
difficulty initiating a bowel movement
excessive straining
a feeling that stool is “stuck” or not moving downward
a sensation of incomplete evacuation
Because this form of constipation reflects a problem with coordination at the outlet of the digestive tract, it is often important to address it directly and early.
If stool cannot be effectively eliminated due to pelvic floor dyssynergia or outlet dysfunction, other supportive measures — such as improving hydration, modifying fiber intake, or optimizing intestinal motility — may provide partial benefit but are often insufficient on their own to fully resolve symptoms.
For this reason, when symptoms suggest difficulty with evacuation or pelvic floor coordination, targeted therapies that address this mechanism are frequently recommended.
One of the most effective first-line approaches is pelvic floor physiotherapy, which focuses on retraining the coordination of the muscles involved in bowel movements. In many cases this therapy uses techniques such as biofeedback to help individuals learn to properly relax and coordinate the pelvic floor during defecation.
Pelvic floor physiotherapy is widely recommended in the management of dyssynergic defecation and other forms of outlet dysfunction, and in some cases may be pursued even before specialized testing such as anorectal manometry.
In some individuals, musculoskeletal or neuromuscular factors involving the pelvis, sacrum, or coccyx may also contribute to difficulties with evacuation or pelvic floor coordination. When these factors are present, manual therapies that address restrictions or dysfunctions in these regions may sometimes be helpful as part of a broader treatment approach.
Some practitioners incorporate osteopathic or visceral manual therapies aimed at improving mobility and neuromuscular coordination within the abdomen and pelvis. While the evidence base for these approaches is more limited than for pelvic floor physiotherapy, they may serve as supportive strategies in selected cases, particularly when structural or neuromuscular factors appear to contribute to symptoms.
Because constipation can arise from different points along the digestive propulsion system, identifying where the breakdown occurs is often the key to choosing the most effective treatment approach.
Major Influences on Coordinated Propulsion in the Gut
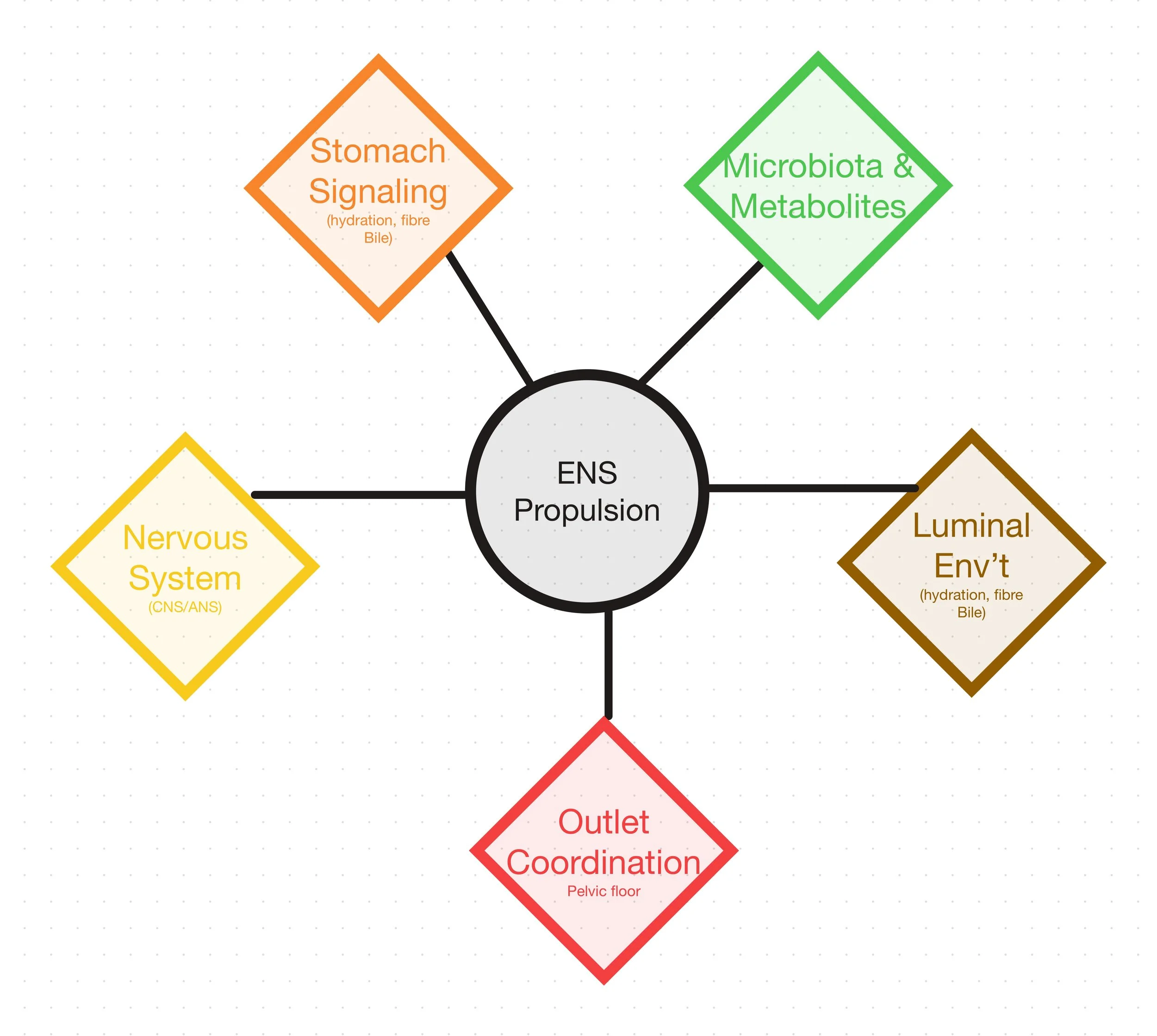
If constipation continues despite efforts to improve diet, hydration, or lifestyle habits, the underlying cause may lie in how different parts of the digestive system are coordinating propulsion. A careful evaluation can often help clarify what is happening and identify the most effective way to restore normal bowel function.